Video
Abstract
Authors: Jedd D. Wolchok, Vanna Chiarion-Sileni, Rene Gonzalez, Jean-Jacques Grob, Piotr Rutkowski, Christopher D. Lao, Charles Lance Cowey, Dirk Schadendorf, John Wagstaff, Reinhard Dummer, Pier Francesco Ferrucci, Michael Smylie, Marcus O. Butler, Andrew Graham Hill, Ivan Marquez-Rodas, John B. A. G. Haanen, Tuba Bas, Wim van Dijck, James Larkin, F. Stephen Hodi; Medical Oncology, Memorial Sloan Kettering Cancer Center, and Weill Cornell Medical College, New York, NY; Oncology Institute of Veneto IRCCS, Padua, Italy; University of Colorado Cancer Center, Denver, CO; Aix-Marseille University, APHM, Hôpital Timone, Marseille, France; Maria Sklodowska-Curie Institute-Oncology Center, Warsaw, Poland; Michigan Medicine, Rogel Cancer Center, University of Michigan, Ann Arbor, MI; Texas Oncology-Baylor Charles A. Sammons Cancer Center, Dallas, TX; Department of Dermatology, University of Essen, Essen, and German Cancer Consortium, Heidelberg, Germany; The College of Medicine, Swansea University, Swansea, United Kingdom; Skin Cancer Center, University Hospital of Zürich, Zürich, Switzerland; European Institute of Oncology–IRCCS, Milan, Italy; Cross Cancer Institute, Edmonton, AB, Canada; Princess Margaret Cancer Centre, Toronto, ON, Canada; Tasman Oncology Research, Southport, QLD, Australia; Medical Oncology, General University Hospital Gregorio Marañón & CIBERONC, Madrid, Spain; Netherlands Cancer Institute, Amsterdam, Netherlands; Bristol Myers Squibb, Princeton, NJ; Bristol-Myers Squibb, Princeton, NJ; The Royal Marsden Hospital NHS Foundation Trust, London, United Kingdom; Dana-Farber Cancer Institute, Boston, MA
Research Funding: Bristol Myers Squibb
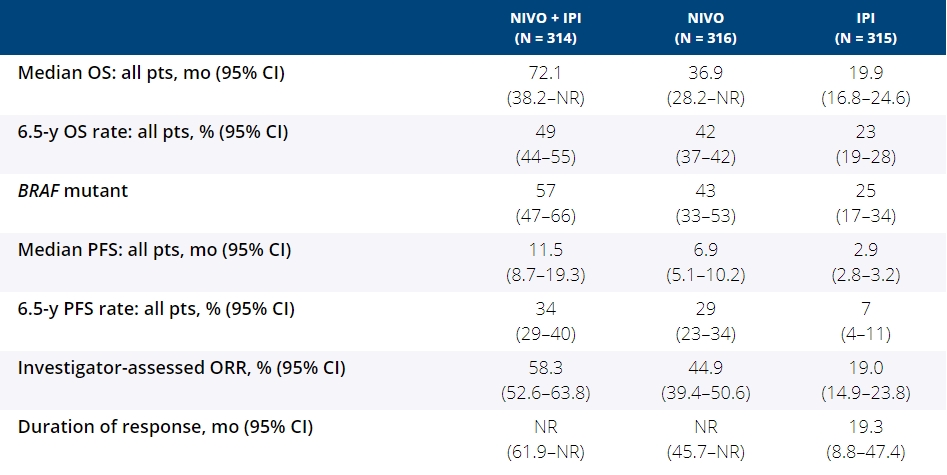
Background: In the phase 3 CheckMate 067 trial, a durable and sustained clinical benefit was achieved with nivolumab (NIVO) + ipilimumab (IPI) and NIVO alone vs IPI at 5-y of follow-up (overall survival [OS] and progression-free survival [PFS] rates: 52%, 44%, 26% and 36%, 29%, 8%, respectively). Here we report 6.5-y efficacy and safety outcomes.
Methods: Eligible pts with previously untreated unresectable stage III or IV melanoma were randomly assigned in a 1:1:1 ratio and stratified by PD-L1 status, BRAF mutation status, and metastasis stage. Pts received NIVO 1 mg/kg + IPI 3 mg/kg for 4 doses Q3W followed by NIVO 3 mg/kg Q2W (n = 314), NIVO 3 mg/kg Q2W + placebo (n = 316), or IPI 3 mg/kg Q3W for 4 doses + placebo (n = 315) until progression or unacceptable toxicity. Co-primary endpoints were PFS and OS with NIVO + IPI or NIVO vs IPI. Secondary endpoints included objective response rate (ORR), descriptive efficacy assessments of NIVO + IPI vs NIVO alone, and safety.
Results: With a minimum follow-up of 6.5 y, median OS was 72.1 mo with NIVO + IPI, 36.9 mo with NIVO, and 19.9 mo with IPI (table). Median time from randomization to subsequent systemic therapy was not reached (NR; 95% CI, 59.6–NR) with NIVO + IPI, 25.2 mo (95% CI, 16.0–43.2) with NIVO, and 8.0 mo (95% CI, 6.5–8.7) with IPI; 36%, 49%, and 66% of pts, respectively, received any subsequent systemic therapy. Median treatment-free interval (which excluded pts who discontinued follow-up prior to initiation of subsequent systemic therapy) was 27.6 mo (range, 0–83.0), 2.3 mo (range, 0.2–81.6), and 1.9 mo (range, 0.1–81.9) with NIVO + IPI, NIVO, and IPI, respectively. Of the pts alive and in follow-up, 112/138 (81%; NIVO + IPI), 84/114 (74%; NIVO), and 27/63 (43%; IPI) were off treatment and never received subsequent systemic therapy; 7, 8, and 0 pts, respectively, were still on treatment. Grade 3/4 treatment-related adverse events were reported in 59% of NIVO + IPI-treated pts, 24% of NIVO-treated pts, and 28% of IPI-treated pts. Since the 5-y analysis, no new safety signals were observed and no additional treatment-related deaths occurred.
Conclusions: This 6.5-y analysis represents the longest follow-up from a phase 3 melanoma trial in the modern checkpoint inhibitor combination therapy and targeted therapy era. The results show durable improved outcomes with NIVO + IPI and NIVO vs IPI in pts with advanced melanoma. We observed improvement in OS, PFS, and ORR with NIVO + IPI over NIVO alone. Clinical trial information: NCT01844505
Slides