Abstract #143 – First Clinical Study of the B-Cell Maturation Antigen (BCMA) 2+1 T Cell Engager (TCE) CC-93269 in Patients (Pts) with Relapsed/Refractory Multiple Myeloma (RRMM): Interim Results of a Phase 1 Multicenter Trial
- Abstract
- Presentation
Author(s)
Luciano J. Costa, MD PhD, Sandy W. Wong, Arancha Bermúdez, Javier de la Rubia, María-Victoria Mateos, Enrique M. Ocio, Paula Rodríguez-Otero, Jesús San-Miguel, Shaoyi Li, Rafael Sarmiento, Pilar Lardelli, Allison Gaudy, Isaac Boss, Lisa M. Kelly, Michael R. Burgess, Kristen Hege, William I. Bensinger
Disclosures
Costa:Fujimoto Pharmaceutical Corporation Japan: Other: Advisor; Karyopharm: Consultancy; Abbvie: Consultancy; Sanofi: Consultancy, Honoraria, Speakers Bureau; GSK: Consultancy, Honoraria, Research Funding; Celgene: Consultancy, Honoraria, Research Funding; Amgen: Consultancy, Honoraria, Research Funding, Speakers Bureau; Janssen: Research Funding, Speakers Bureau. Wong:Genentech: Research Funding; Janssen: Research Funding; Celgene Corporation: Research Funding; Fortis: Research Funding; Juno: Research Funding. Bermúdez:MSD: Consultancy, Speakers Bureau; Amgen: Consultancy, Membership on an entity’s Board of Directors or advisory committees; Janssen: Membership on an entity’s Board of Directors or advisory committees; Fresenius: Consultancy, Membership on an entity’s Board of Directors or advisory committees; Celgene Corporation: Consultancy, Membership on an entity’s Board of Directors or advisory committees, Speakers Bureau. de la Rubia:AMGEN: Consultancy; Celgene Corporation: Consultancy; AbbVie: Consultancy; Takeda: Consultancy; Janssen: Consultancy. Mateos:Pharmamar: Membership on an entity’s Board of Directors or advisory committees; Takeda: Honoraria, Membership on an entity’s Board of Directors or advisory committees; Adaptive: Honoraria; EDO: Membership on an entity’s Board of Directors or advisory committees; GSK: Membership on an entity’s Board of Directors or advisory committees; Abbvie: Membership on an entity’s Board of Directors or advisory committees; Celgene: Honoraria, Membership on an entity’s Board of Directors or advisory committees; Janssen: Honoraria, Membership on an entity’s Board of Directors or advisory committees; Amgen: Honoraria, Membership on an entity’s Board of Directors or advisory committees. Ocio:BMS: Honoraria; Sanofi: Research Funding; Mundipharma: Research Funding; Takeda: Consultancy, Honoraria; Seattle Genetics: Consultancy; Celgene: Consultancy, Honoraria, Research Funding; Array Pharmaceuticals: Research Funding; Pharmamar: Consultancy; Novartis: Consultancy, Honoraria; AbbVie: Consultancy; Amgen: Consultancy, Honoraria, Research Funding; Janssen: Consultancy, Honoraria. Rodríguez-Otero:Celgene Corporation: Consultancy, Honoraria, Speakers Bureau; Janssen: Consultancy, Honoraria; Takeda: Consultancy; BMS: Honoraria; Kite Pharma: Consultancy. San-Miguel:Amgen, Bristol-Myers Squibb, Celgene, Janssen, MSD, Novartis, Roche, Sanofi, and Takeda: Consultancy, Honoraria. Li:Celgene Corporation: Employment, Equity Ownership. Sarmiento:Celgene Corporation: Employment. Lardelli:Celgene Corporation: Employment, Equity Ownership. Gaudy:Celgene Corporation: Employment, Equity Ownership. Boss:Celgene Corporation: Employment, Equity Ownership. Kelly:Celgene Corporation: Employment. Burgess:University of California: Other: Volunteer clinical faculty, without salary, Patents & Royalties: Patent – T315A and F317I mutations of BCR-ABL kinase domain; Celgene Corporation: Employment, Equity Ownership, Patents & Royalties: Patent – CD47 antibodies and methods of use thereof. Hege:Celgene Corporation: Employment, Equity Ownership, Patents & Royalties; Arcus Biosciences: Membership on an entity’s Board of Directors or advisory committees; Society for Immunotherapy of Cancer: Membership on an entity’s Board of Directors or advisory committees; Mersana Therapuetics: Membership on an entity’s Board of Directors or advisory committees. Bensinger:Amgen, Celgene: Other: Personal Fees, Research Funding, Speakers Bureau; Takeda, Janssen: Speakers Bureau; Sanofi, Seattle Genetics, Merck, Karyopharm: Other: Grant.
Introduction
BCMA is a tumor necrosis factor (TNF) receptor superfamily transmembrane glycoprotein essential for the maturation and survival of plasma cells. CC-93269 is an asymmetric 2-arm humanized IgG TCE that binds bivalently to BCMA and monovalently to CD3ε in a 2+1 format (Seckinger A, et al. Cancer Cell. 2017;31:396-410). The CC-93269-mediated interaction between T cells and BCMA-expressing myeloma cells induces T cell receptor/CD3 crosslinking leading to T cell activation, and release of proinflammatory cytokines and cytolytic enzymes, resulting in myeloma cell death. In preclinical studies with CC-93269 and related molecules, 2+1 BCMA TCEs induced tumor regression in animal models and promoted myeloma cell death in primary pt myeloma cells. Here we report interim results from a phase 1 dose-finding study (CC-93269-MM-001; NCT03486067) evaluating CC-93269 in pts with RRMM.
Methods
Eligible pts had RRMM and had received ≥ 3 prior regimens without prior BCMA-directed therapy. In dose escalation, CC-93269 was administered intravenously over 2 hours on Days 1, 8, 15, and 22 for Cycles 1-3; Days 1 and 15 for Cycles 4-6; and on Day 1 for Cycle 7 and beyond, all in 28-day cycles. Dose escalation involved 2 stages: in stage 1, CC-93269 was given in fixed doses; in stage 2, pts received a fixed first dose on Cycle 1 Day 1, followed by intrapatient dose escalation on Cycle 1 Day 8. Primary objectives were to assess the safety and tolerability of CC-93269 and define the maximum tolerated dose (MTD), non-tolerated dose (NTD), and/or recommended phase 2 dose (RP2D). Minimal residual disease (MRD) was assessed after clinical response in pt bone marrow aspirate samples by Next Generation Flow using the EuroFlow panel. MRD negativity was reported only if a minimum sensitivity of < 1 tumor cell in 105 nucleated cells was achieved.
Results
As of May 24, 2019, 19 pts had received CC-93269. Median age was 64 years (range 51-78), with a median of 6.2 years (range 1.4-13.9) since initial diagnosis. The median number of prior regimens was 6 (range 3-12) and included treatment with autologous stem cell transplantation (73.7%), allogenic stem cell transplantation (10.5%), lenalidomide (100%), pomalidomide (84.2%), bortezomib (100%), carfilzomib (84.2%), and daratumumab (DARA; 94.7%). All pts had MM refractory to their last line of therapy, with 16 (88.9%) refractory to DARA, 17 (89.5%) to their last proteasome inhibitor, and 16 (84.2%) to their last immunomodulatory agent.
CC-93269 doses ranged from 0.15 to 10 mg; median duration of treatment was 14.6 weeks (range 1.6-32.0) with pts receiving a median of 4 cycles (range 1-8). Grade 3-4 treatment-emergent adverse events were reported in 15 (78.9%) pts and included 10 (52.6%) pts with neutropenia, 8 (42.1%) with anemia, 5 (26.3%) with infections, and 4 (21.1%) with thrombocytopenia. No pt required dose modifications. Cytokine release syndrome (CRS) was reported in 17 (89.5%) pts, the majority of whom reported a maximum grade 1 (n = 11 [57.9%]) or grade 2 (n = 5 [26.3%]), and occurred most frequently with the first or second dose (n = 22 of 27 events [81.5%]). CRS prophylaxis was implemented with dexamethasone for first dose and dose increases in pts receiving ≥ 6 mg. Of 27 CRS events, 8 (29.6%) were managed with dexamethasone and 10 (37.0%) with tocilizumab. One pt receiving 6 mg CC-93269 as first dose and 10 mg on Cycle 1 Day 8 died on study in the setting of CRS, with a potential infection as a contributing factor. Dose-related pharmacodynamic activity, including peripheral blood immune cell redistribution and transient release of pro- and anti-inflammatory cytokines, was observed in pts.
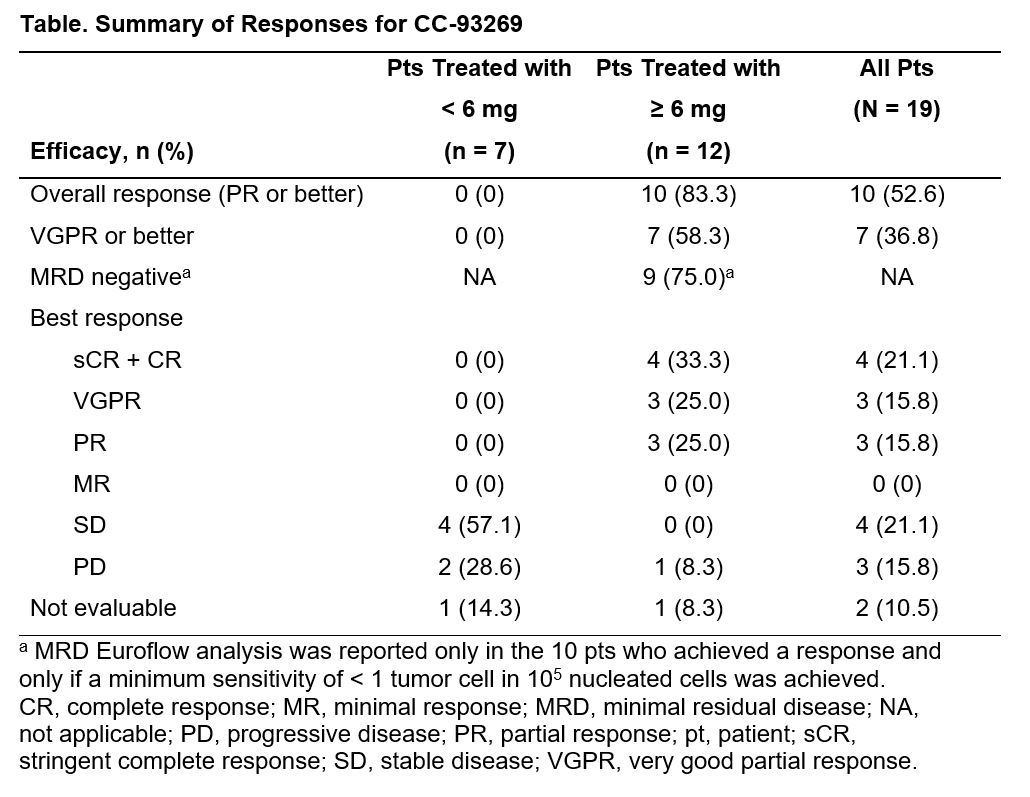
Of the 12 pts treated with ≥ 6 mg CC-93269 in Cycle 1, 10 pts achieved a partial response (PR) or better (overall response rate; 83.3%), including 7 (58.3%) with a very good partial response (VGPR) or better and 4 (33.3%) with a stringent complete response (sCR) (Table); 9 (75.0%) pts achieved MRD negativity. The median time to response was 4.2 weeks (range 4.0-13.1), and 10 of 10 responses were ongoing with follow-up ranging from 2.1 to 4.7 months. The NTD, MTD, and RP2D have not yet been reached.
Conclusions
CC-93269, a 2+1 BCMA TCE, shows a manageable safety profile and promising efficacy, including MRD-negative sCRs, in pts with heavily pretreated RRMM. The study continues to enroll in the dose escalation phase. Updated safety and efficacy data will be presented at the meeting.
Oral Abstract
© 2020 American Society of Hematology. All rights reserved.
Meeting: 2019 ASH Annual Meeting
Presenter(s): Luciano Costa et al.
Presentation Date: December 9, 2019
Abstract #: 143
Disclaimer
© 2020 American Society of Hematology. All rights reserved. ASH® and the ASH logo are registered trademarks of the American Society of Hematology. Used with permission.
This content is provided for informational purposes and personal use only, and is not intended to provide medical advice, diagnosis, or treatment or for commercial use. The ideas and opinions expressed herein do not necessarily reflect those of the American Society of Hematology (ASH®). The mention of any product, service or therapy in this collection of materials should not be construed as an endorsement of the products mentioned.
Copyright © 2020 Springer Healthcare Limited. Part of the Springer Nature Group.
